SPECIAL SEMINAR:
DIAGNOSTIC PEARLS IN
SURGICAL PATHOLOGY,
WITH EMPHASIS ON MEDIASTINAL TUMORS
Juan Rosai (Milàn, Italia)
Saul Suster (Milwaukee, USA)
Saturday, May 23, 2009
CLINICAL HISTORIES
CASE 1 (Dr. Suster)
A 45-year-old woman was seen for symptoms of dyspnea and chest pain. A
chest X-ray and CT scan showed a 15 cm. anterior mediastinal mass. Past
history revealed a status post-mastectomy for invasive ductal carcinoma
of the breast 3 years ago and a hysterectomy for “uterine fibroids” 5
years ago.

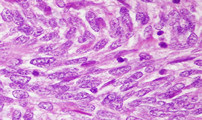
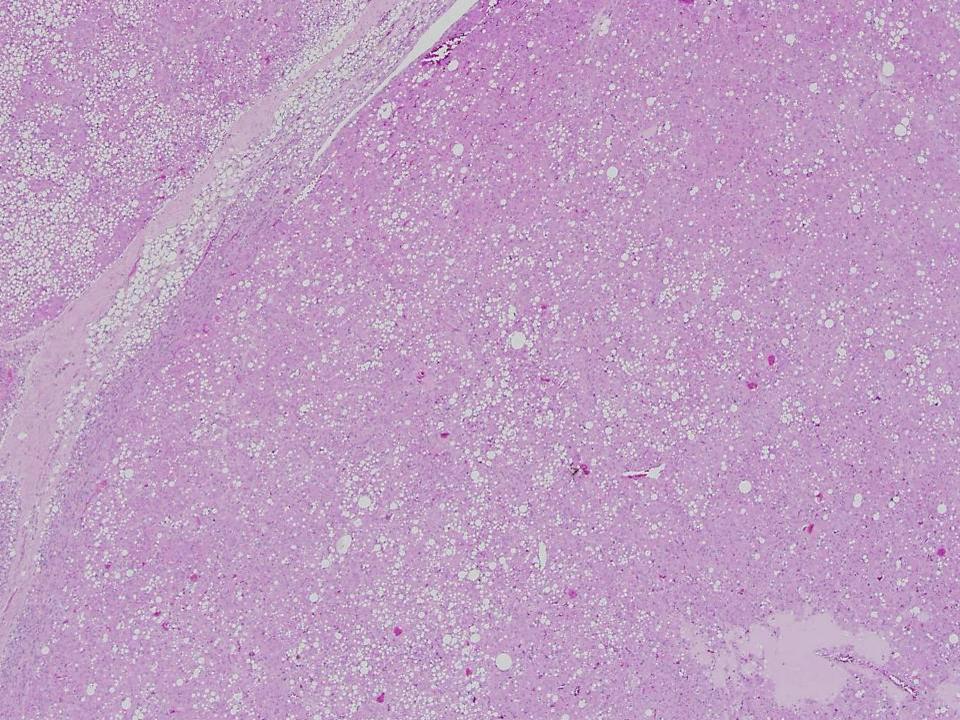
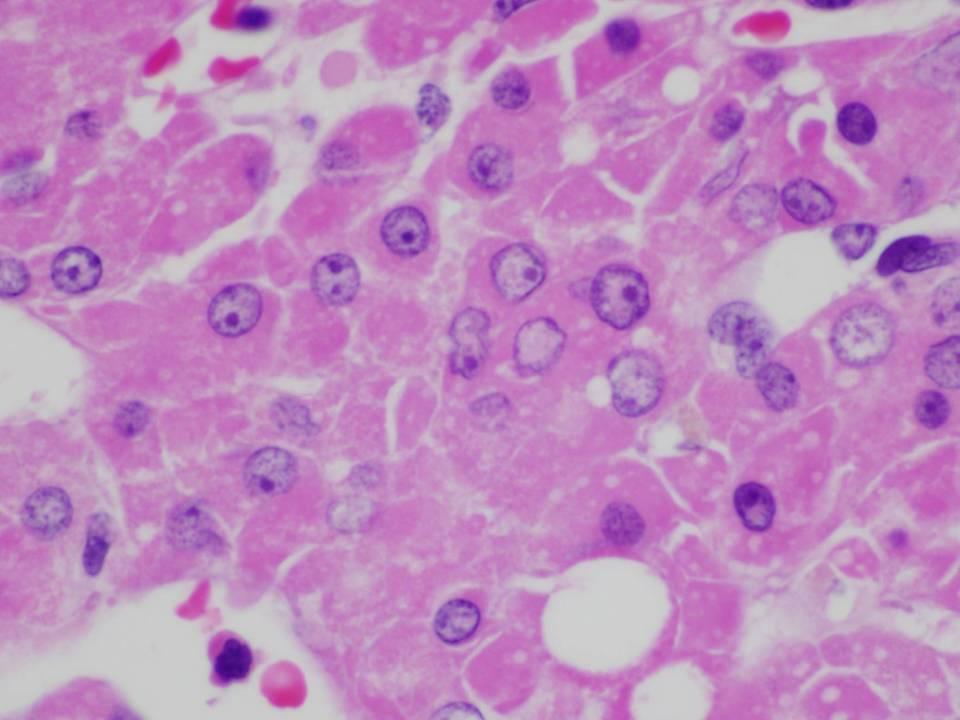
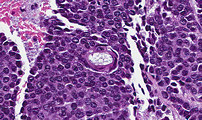
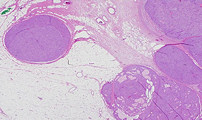
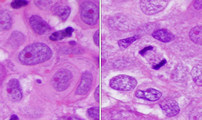
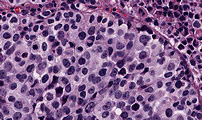
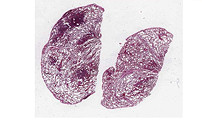
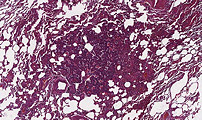
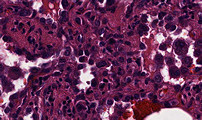
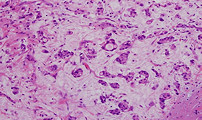
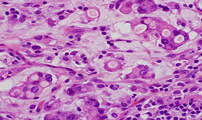
CASE 2 (Dr. Rosai)
A 77-year-old woman with a history of rheumatic polymyalgia and diffuse
arteritis with spontaneous fracture of one femur one year previously (attributed
to osseous infarct) presented with abdominal pain, sickness, vomiting,
choluria, and cutaneous rash in the arms. On admission, the patient had
elevated levels of serum CA125 (34U/mL) and alphafetoprotein (25,990 μg/L).
Ultrasonography and CT scan showed a polylobated mass measuring 9,5 x 9
x 10 cm in the region of the head of the pancreas, associated with
enlarged peripancreatic and supraclavicular lymph nodes. One of the
latter was biopsied. The microscopic images are from this specimen. An
additional CT scan taken 10 days after the biopsy showed multiple
bilateral lung nodules consistent with metastases. No metastases were
detected in the liver or other sites. The patient deteriorated quickly
and died of tumor one year after the initial visit.
CASE 3 (Dr. Suster)
A 65-year-old man was seen because chest pain and shortness of breath. A
CT scan showed a 15 cm. anterior mediastinal mass. The lung fields were
clear and free of tumor, and the only significant past history of the
patient was a myocardial infarct at age 62 due to atherosclerotic
coronary disease.
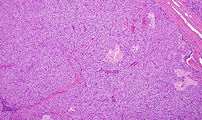
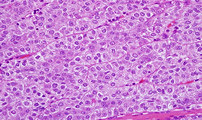
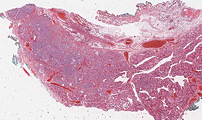
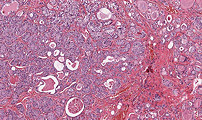
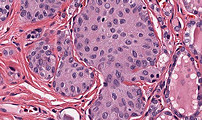
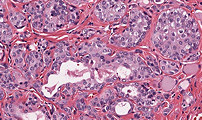
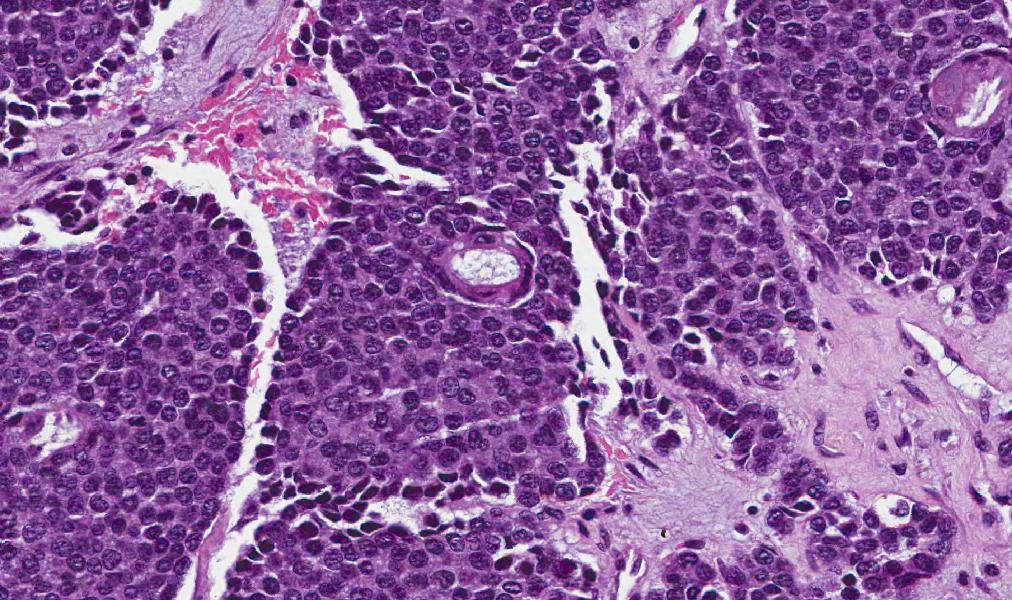
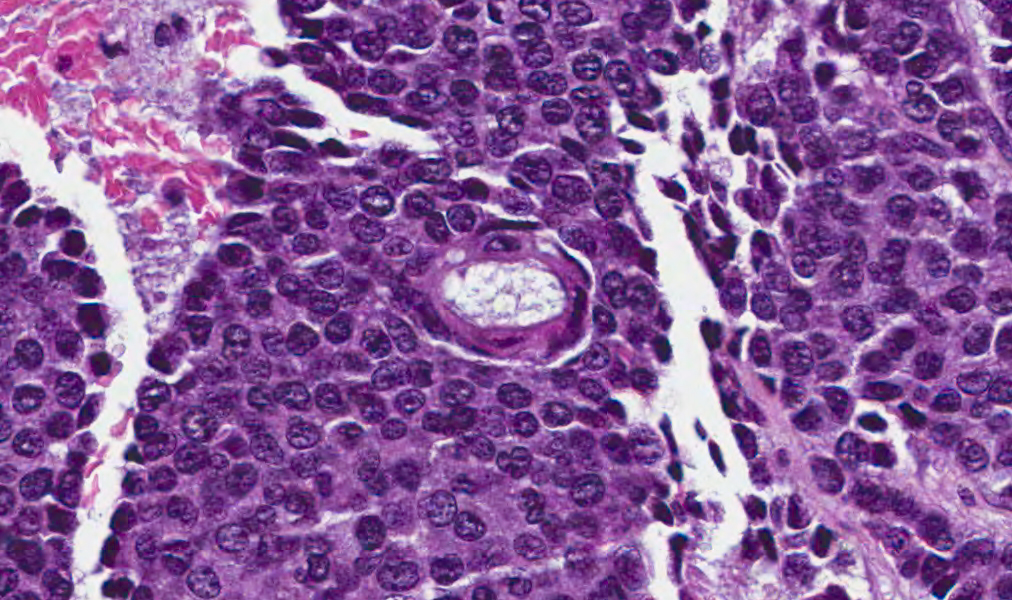
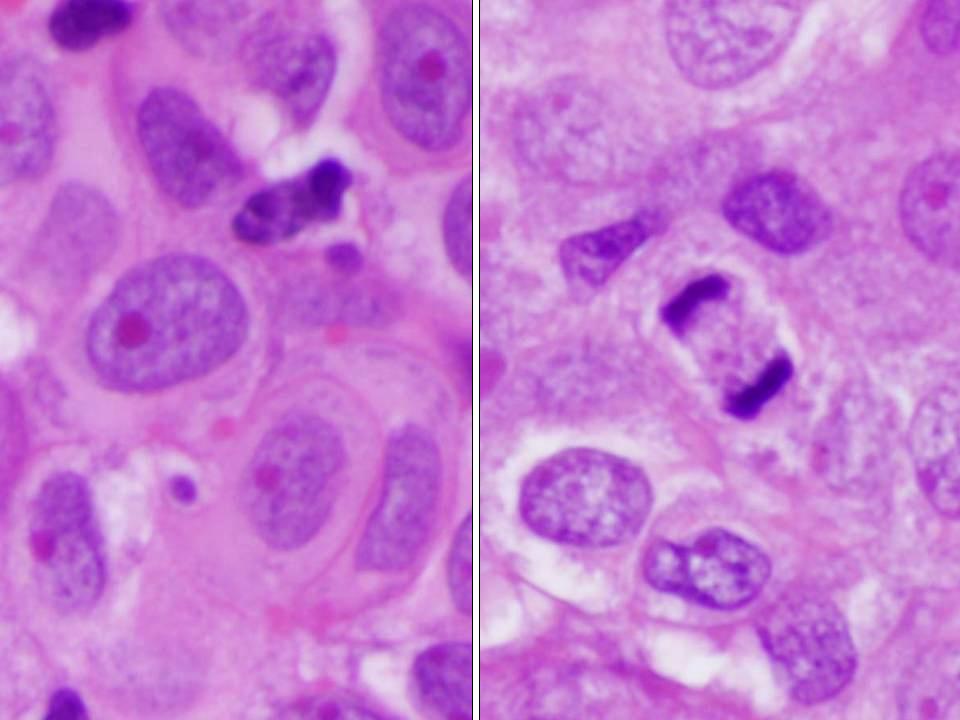
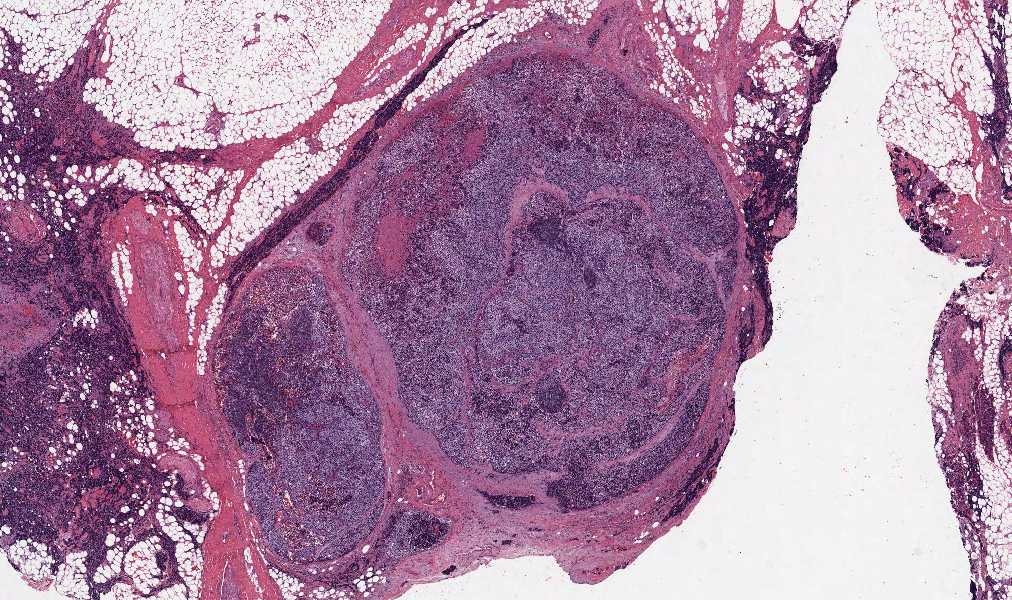
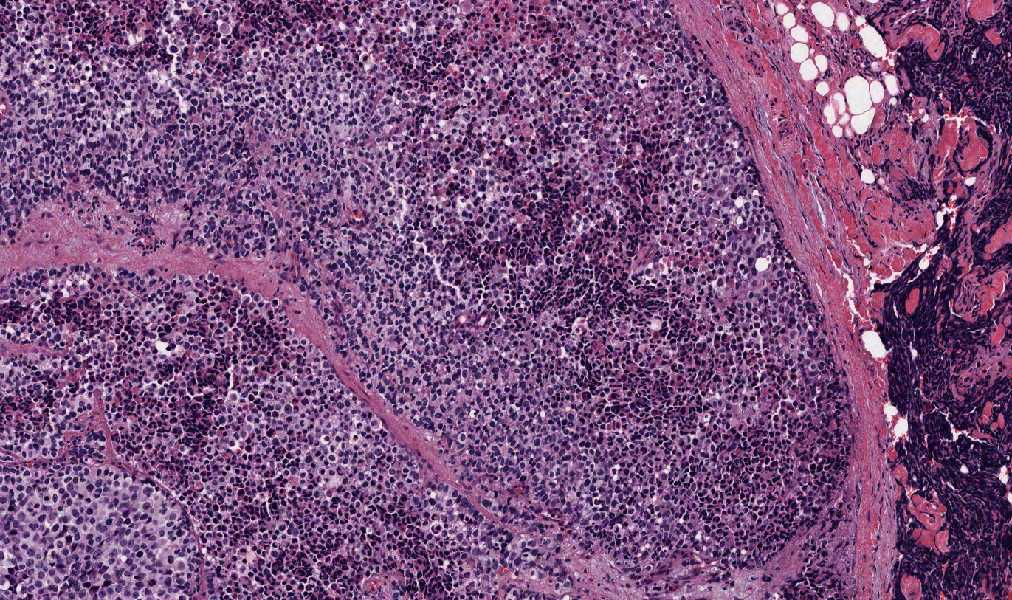
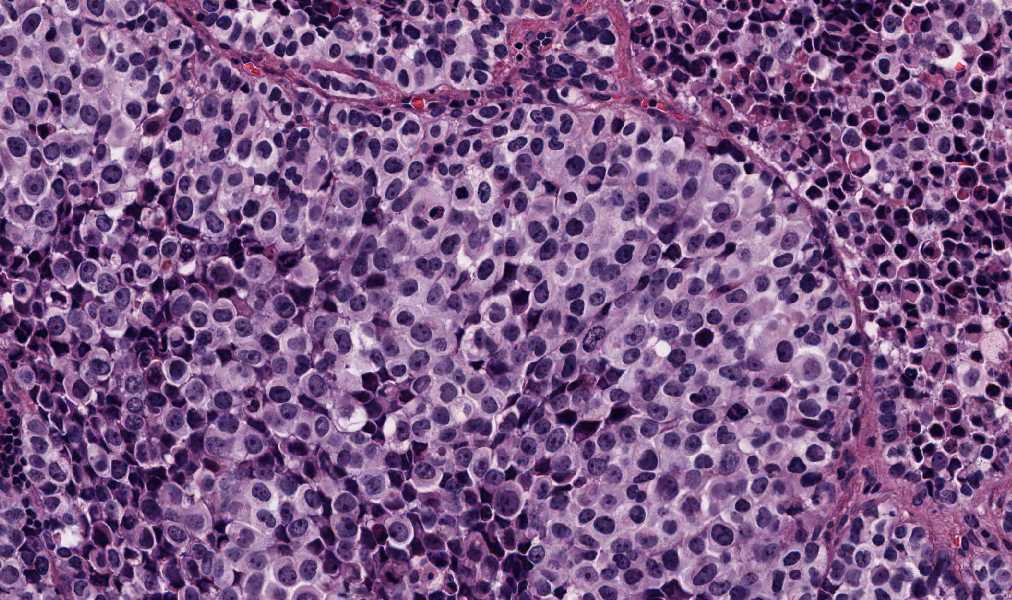
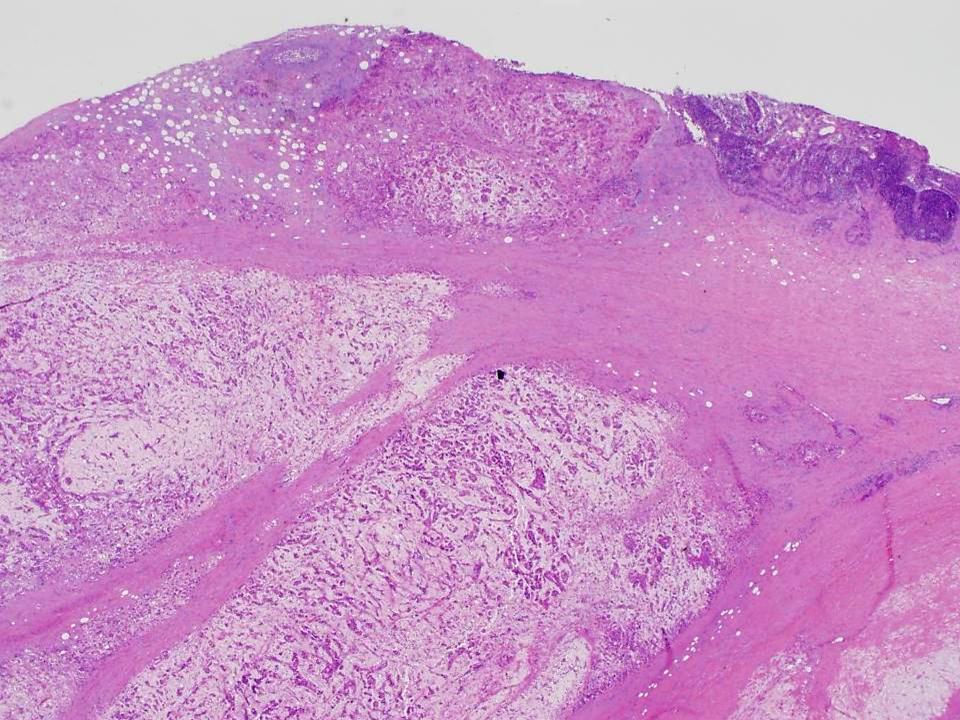
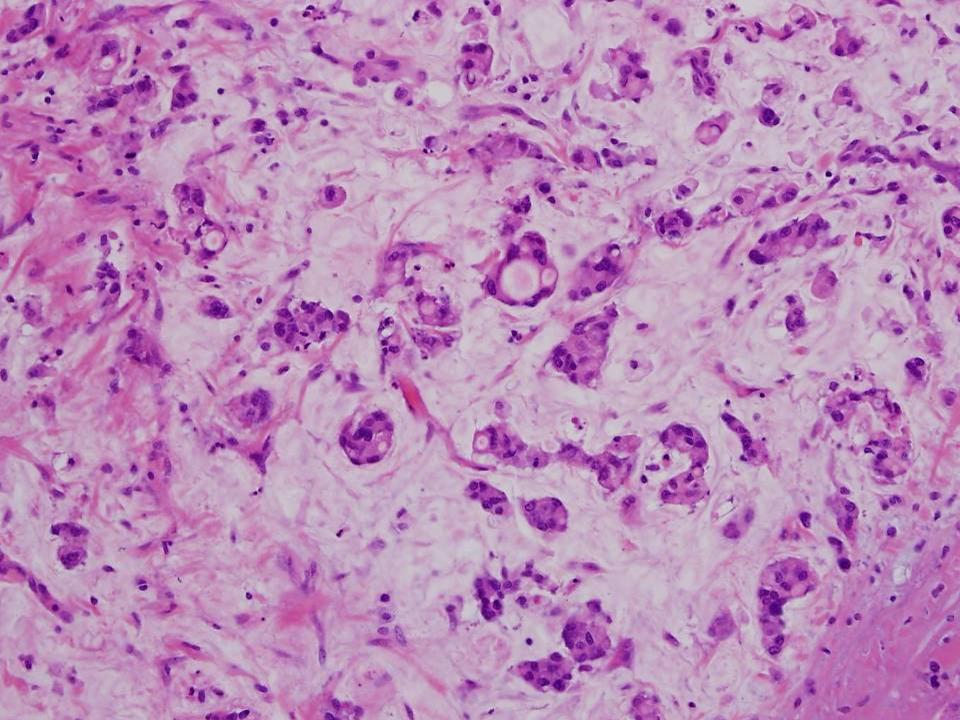
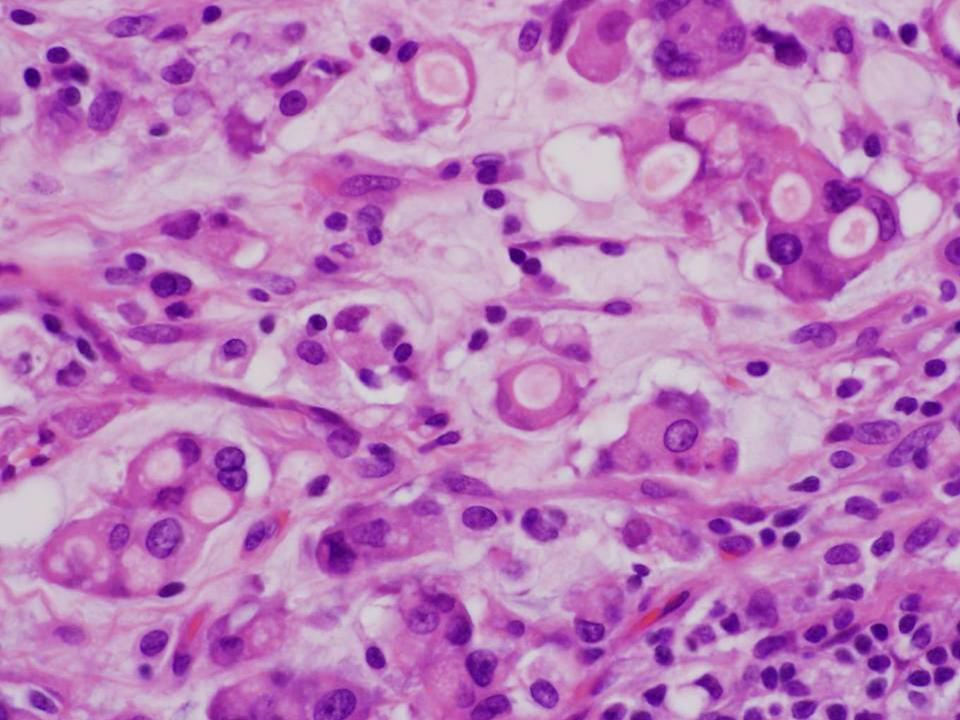
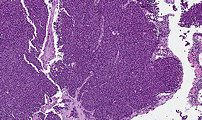
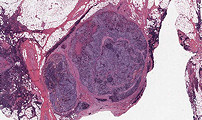
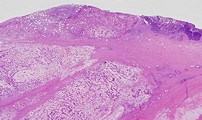
CASE 4 (Dr. Rosai)
A 65-year-old female presented with multiple right cervical
lymphadenopathy. She had a past history of invasive ductal carcinoma of
the right breast. The thyroid was clinically unremarkable. One of the
cervical lymph nodes was biopsied. The images submitted are from the
lymph node lesion. On further lincial examination, a large mass was
found in the nasal cavity.
CASE 5 (Dr. Suster)
A 17-year-woman was seen for shortness of breath and chest pain. A CT
scan of the chest showed a 12x10x8 cm well-circumscribed anterior
mediastinal mass. There was no significant previous history or evidence
of tumor elsewhere on radiographic and physical examination.
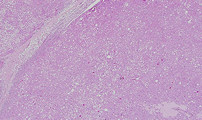
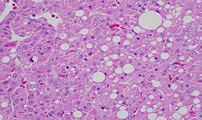
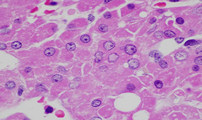
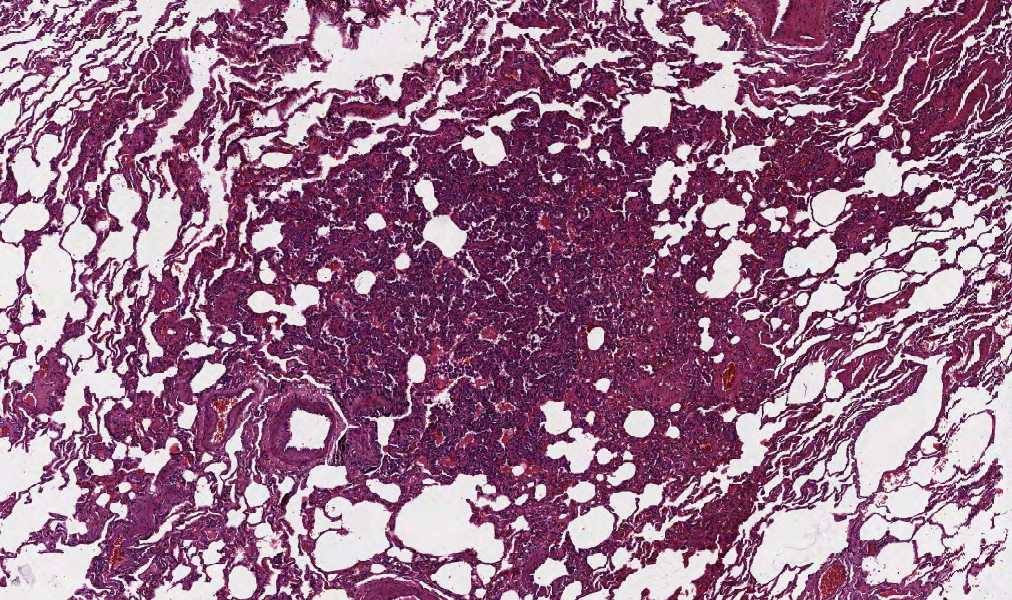
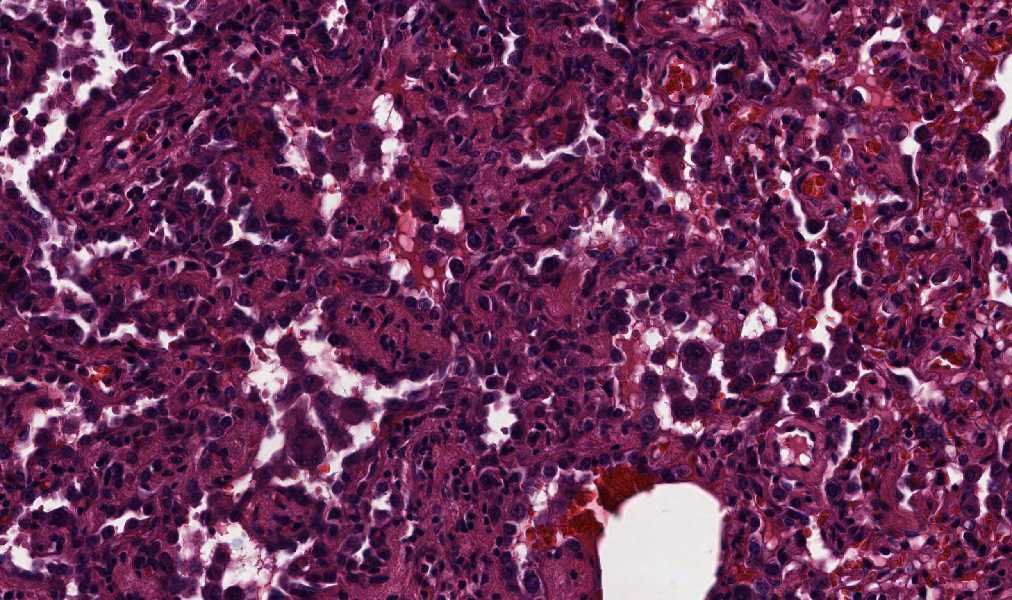
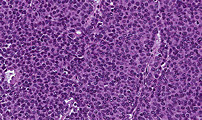
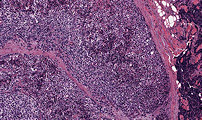
CASE 6 (Dr. Rosai)
A 51-year-old male was found to have multiple bilateral small pulmonary
nodules on chest CT scan. There was a history of hemicolectomy for a
combined adenocarcinoma–small cell neuroendocrine carcinoma of the colon
one year previously. A partial resection of lung tissue containing
several nodules was carried out. The images shown are from the lung
specimen.

CASE 7 (Dr. Suster)
A 58-year-old man was admitted to the hospital because of chest pain.
Imaging studies showed a 15 cm. anterior mediastinal mass. The lung
fields were clear and free of tumor. The patient had no history of
previous malignancy or evidence of tumor elsewhere.
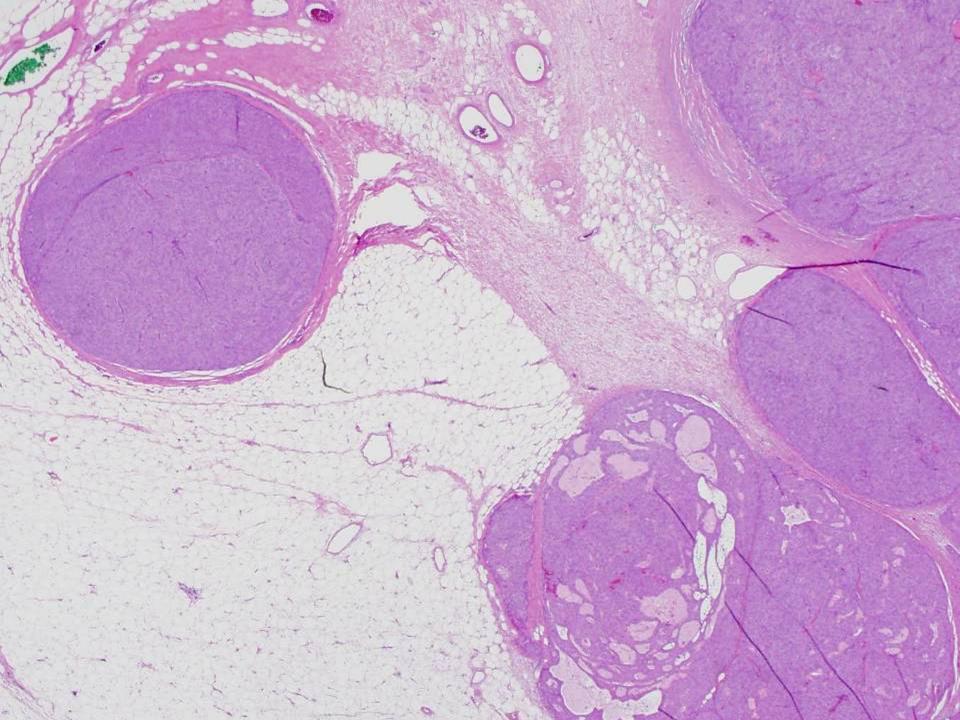
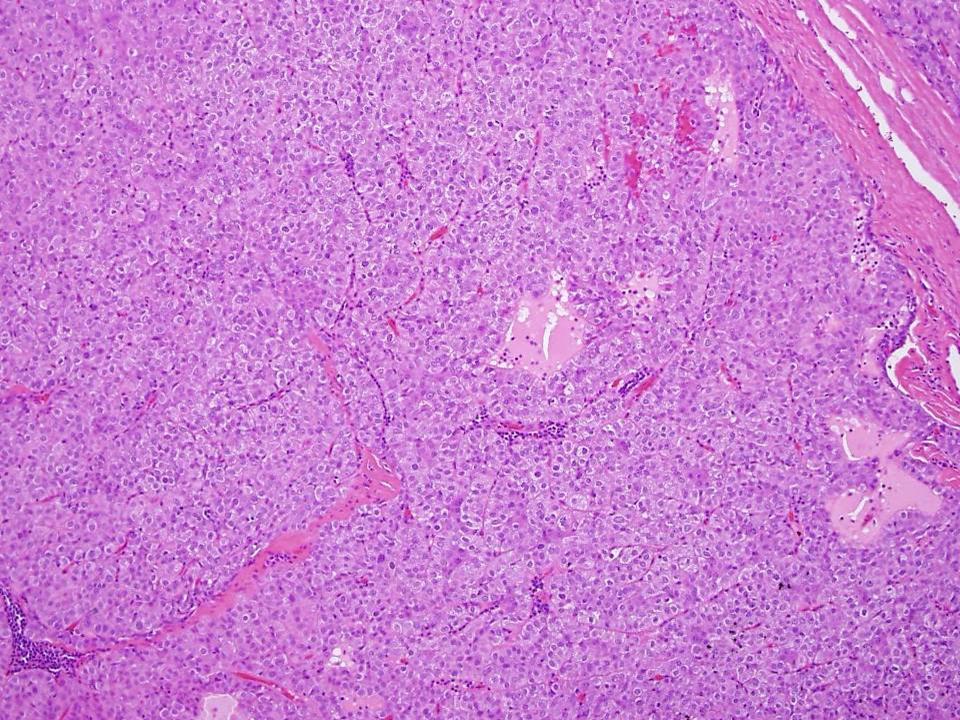
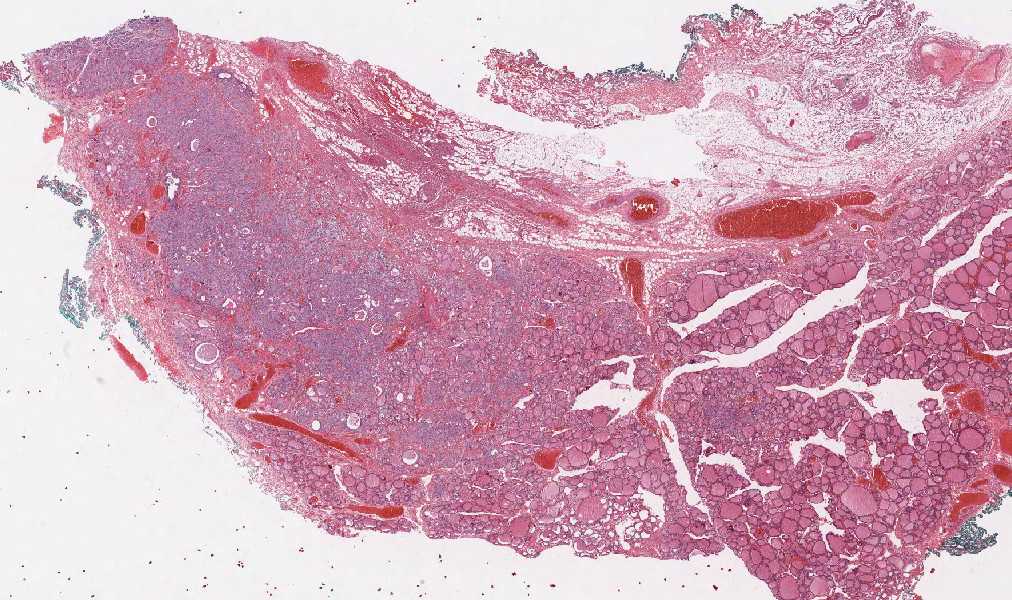
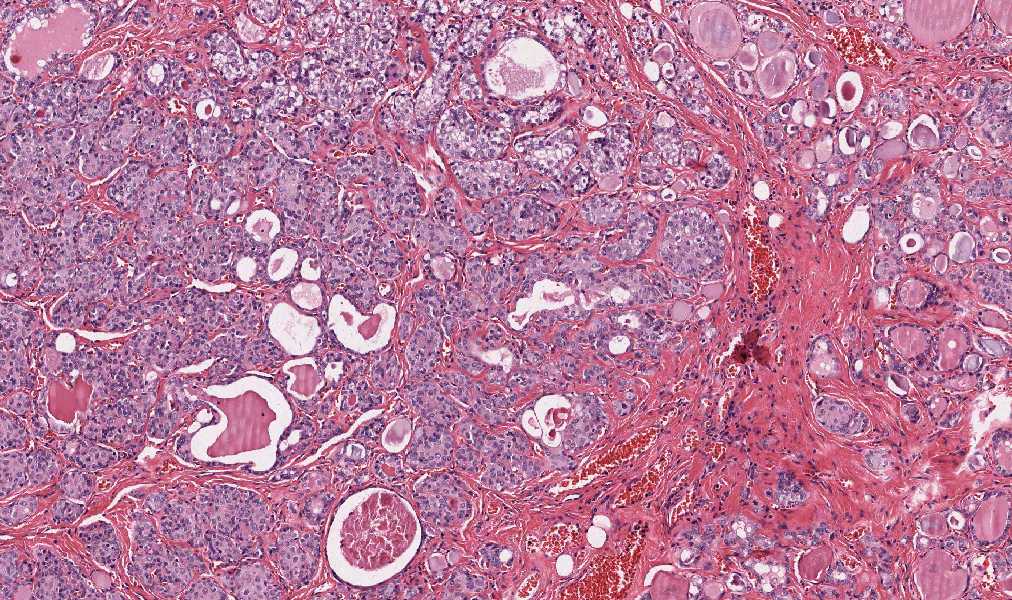
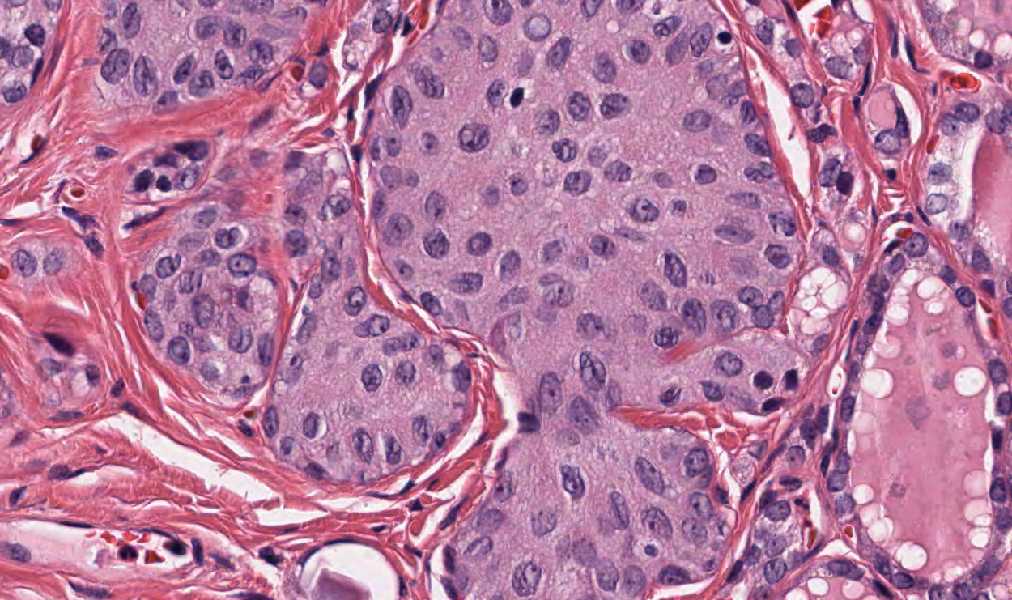
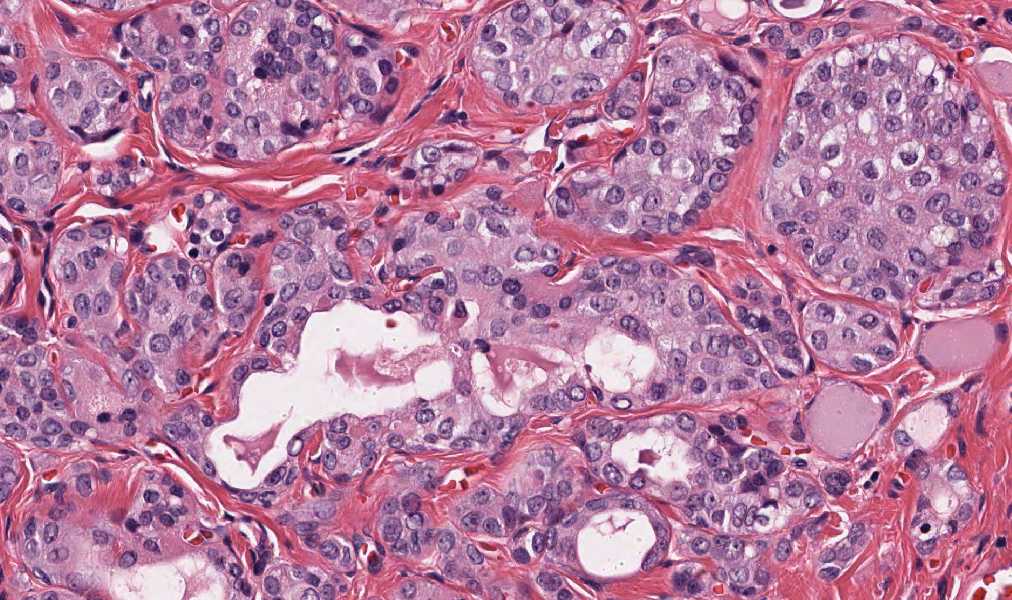
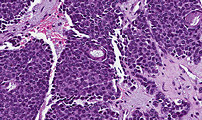
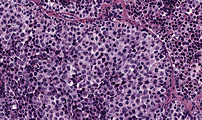
CASE 8 (Dr. Rosai)
A 50-year-old male was found to have a mild but persistent elevation of
serum calcitonin levels (up to 23 pg/ml), identified during a work-up
for irritable bowel syndrome. Endocrinologic work-up did not provide an
explanation for this abnormality, except for the presence of a 3 mm
thyroid nodule found on ultrasound. Clinically, the thyroid was not
palpable and there was no cervical lymphadenopathy. The patient was
advised to have a total thyroidectomy because of the risk of medullary
carcinoma. Grossly, the thyroid was somewhat nodular but without obvious
tumor.